-1.png?width=431&height=115&name=Untitled%20design%20(2)-1.png)
.png)

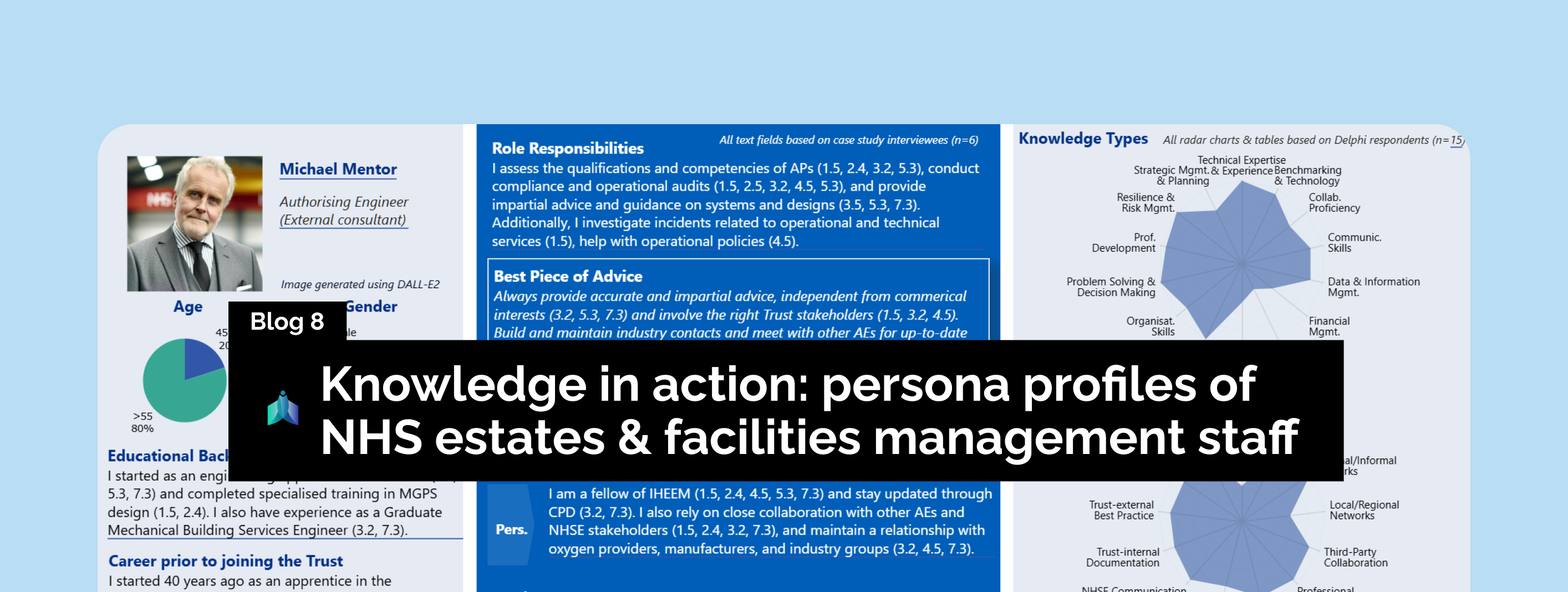
The NHS is one system. Everyone has an NHS email address. Everyone works for the same ultimate goal: patient care. Yet staff in one hospital can't easily get in touch with their counterparts just down the road.
An engineer dealing with a complex ventilation problem at one Trust has no simple way to contact someone who solved the same issue at another Trust last month.
You might assume this is about IT systems or organisational silos. It's not. My research across multiple NHS Trusts reveals something more personal: social and human barriers that prevent experienced staff from learning from each other.
My research across multiple NHS Trusts - including case studies and a Delphi survey of 165 EFM professionals - reveals a quiet but systemic breakdown in knowledge sharing. The core problem isn’t technical.
It’s human.
Five core social barriers are stopping experienced staff from learning from each other, and they’re quietly eroding resilience, safety, and efficiency across the NHS estate.
Barrier 1: The myth of competition
Early on in my research, various people pointed out that one of the key barriers to knowledge sharing are competitive dynamics between NHS Trusts. However, less than one in five participants actually see competition as a barrier to knowledge sharing. One Manager reflected: "where does this come from, I've never experienced this." Another stated there's "no competition - we are squarely the weak partner to our local Acute Trust."

Figure 1: Competition is not the barrier we think it is
Instead, what looks like competition is often just organisational self-preservation. As one Head of EFM explained: “You always look after your own Trust.”
That’s not rivalry. That’s survival instinct in a resource-stretched system.
Barrier 2: The time trap
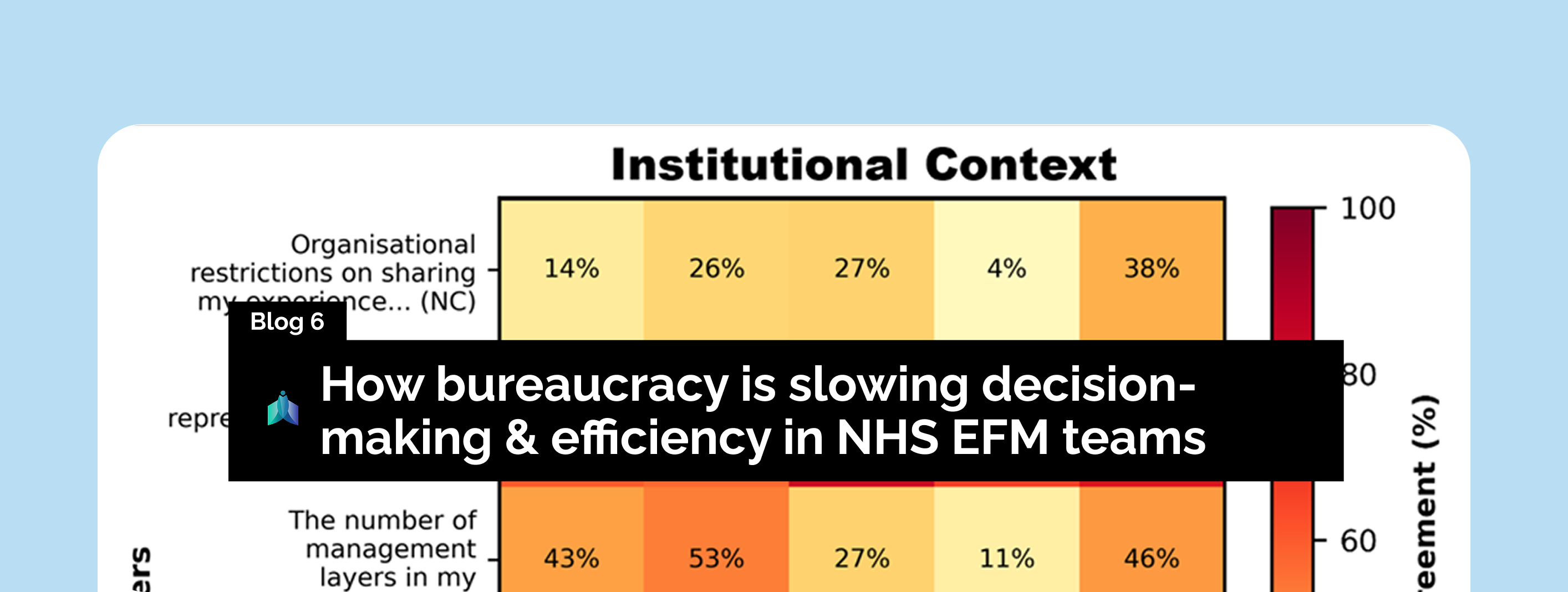
Time is the number one barrier to knowledge sharing - and it hits hardest where operational complexity is highest. 85% of AEs and 81% of Managers report excessive workload. 91% of Heads of EFM report being pulled between strategy and firefighting. 65–82% across all roles say they lack time to reflect on recurring issues.

Figure 2: Lack of time is the top barrier to knowledge sharing
One Manager put it bluntly: “There’s too much daily to keep on top of what’s required as a minimum.” - leaving zero capacity for knowledge sharing. Meanwhile, APs often hold "multiple AP appointments" whilst being expected to mentor others across multiple Trusts.
This creates another vicious cycle: the people with the most experience, insight, and oversight don’t have time to share what they know, and the system gets weaker as a result.
Barrier 3: AEs view lacking competency as a critical barrier
This should ring alarm bells: 100% of Authorising Engineers (AEs) in my study flagged major competency issues in the NHS EFM workforce.
Yet only 22% of Directors of EFM saw the same problem.
That’s a huge reality gap.
AEs are not just technical advisors - they formally assess the competency of Authorised Persons, who manage critical systems like water, ventilation, and medical gases. When AEs see systemic gaps, it’s not a complaint. It’s a professional audit.
 Figure 3: The reality gap: AEs see what others miss
Figure 3: The reality gap: AEs see what others miss
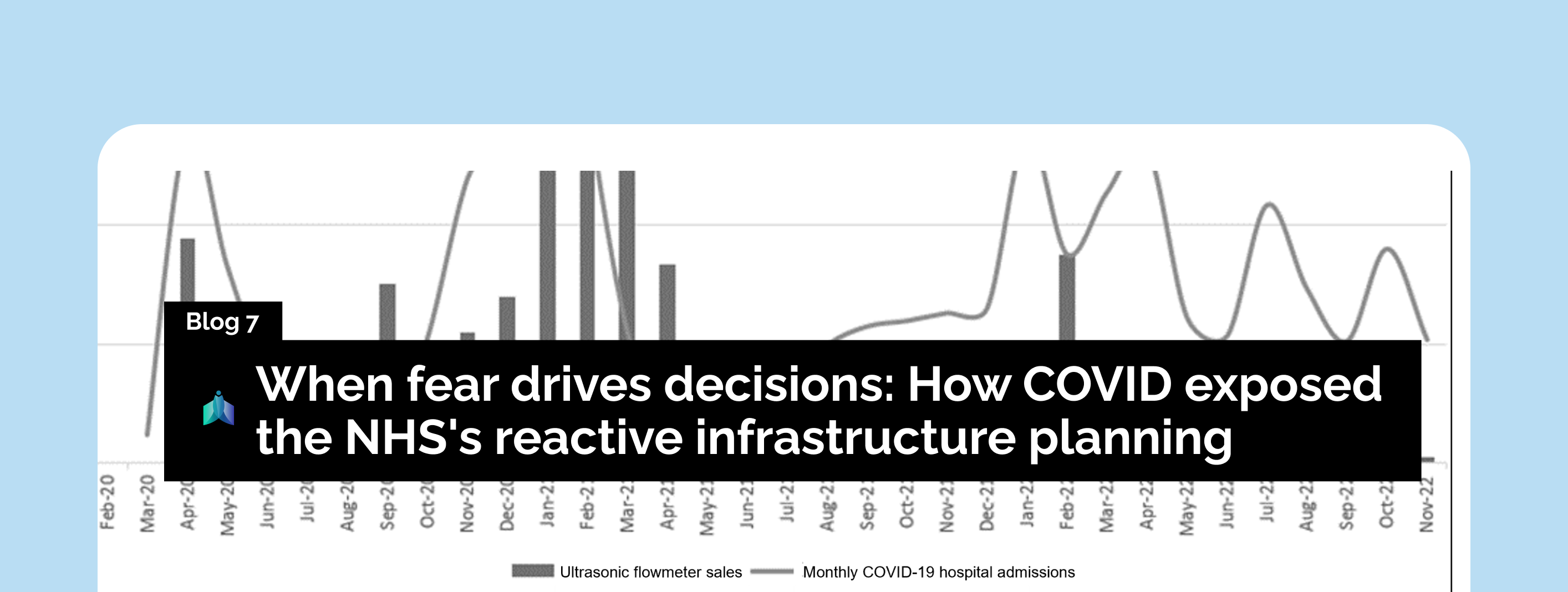
And during COVID-19, the weaknesses became impossible to ignore. AEs described that APs were "often responsible for multiple disciplines" and "were unable to adequately relate and apply external knowledge to their local context". Some Trusts were so desperate they recalled retired staff - showcasing how we've allowed institutional knowledge to leave the system without replacement.
Barrier 4: Directors network, middle managers don't
Directors of EFM move in well-connected circles. Most attend conferences, sit on committees, and build relationships over years of career progression. When faced with a new challenge, they know someone who can advise or "make connections as needed".

Figure 4: The networking divide: Senior staff connect, middle management struggles
But Managers (including APs) and Heads of EFM don't enjoy the same luxury. The majority struggle with something seemingly basic: they don't have contact details for peers in other Trusts. These are the people actually running day-to-day operations, yet they're operating in professional isolation.
The problem isn't just about seniority - it's about opportunity. As outlined in blog post #3, middle management roles are overloaded with tasks delegated down from above. Whilst Directors attend networking events and industry conferences, Managers and Heads of EFM are buried in operational demands, never getting the chance to build the peer relationships they desperately need.
One Head of EFM suggested a simple solution: "a national index of colleagues working in EFM". It's almost remarkable that in 2025 we need to spell out something so fundamental. IHEEM is now doing something about this. They are working on establishing an AP list - critical infrastructure that could transform how knowledge flows through the NHS.
But contact lists only solve part of the problem. "Frequent movement of senior managers amongst organisations" constantly disrupts what networks do exist. One interviewee spends considerable time just "locating responsible individuals in other Trusts".
Previously, regional programmes allowed visits and direct interaction between Trusts. These disappeared due to "time constraints" - short-term savings that created massive long-term knowledge deficits.
Barrier 5: Recognition matters more than most people think
“Just a socket on the wall.”That’s how one NHS AP described how others view EFM. Clinical teams often miss the complexity behind what looks simple. And the NHS’s own communication doesn’t help - EFM teams are still classed as Maintenance & Ancillary in staff surveys, not as the critical infrastructure specialists they are.

Figure 5: Job satisfaction across EFM roles reveals a clear appreciation gap - the majority of Heads and Directors feel services are undervalued.
When 82% of Heads of EFM and 62% of Directors say their teams feel unappreciated, it’s not just about pride. It’s about performance.
As Lord Carter of Coles put it, the EFM workforce is “too often seen as a cost to control, not a productive asset to harness.”
That mindset erodes job satisfaction and stifles collaboration. When staff feel undervalued, they’re less likely to share knowledge or connect across teams, making EFM look reactive rather than strategic. It’s a vicious cycle of invisibility.
During COVID-19, clinical and EFM teams forged closer bonds (more on that in future posts). Crises made everyone more aware of each other’s value. But many EFM professionals say that recognition faded just as quickly once the immediate threat passed.
The bigger picture
The NHS doesn’t have a competition problem. It has a connection problem.
And that connection is being blocked by five quiet, human barriers: Lack of time. Gaps in trust. Professional isolation. Systemic undervaluing. And the reality that the busiest people are the least supported to share what they know.
At INNEX, we're working to rebuild this infrastructure - connecting people, knowledge, and systems so critical insights reach the right hands at the right time. Because the next crisis is likely just around the corner.
Want to dig into the details? Read pages 190-195 in the full thesis here.